Attention Members: Please avoid clicking on any unsolicited emails with attachments. If you have any concerns, please contact us at info@veteducation.com.au for clarification.
Attention Members: Please avoid clicking on any unsolicited emails with attachments. If you have any concerns, please contact us at info@veteducation.com.au for clarification.
Haemostasis necessitates an appropriate balance between the coagulation cascade that produces a fibrin clot and the fibrinolytic system that dissolves a fibrin clot1.
In patients with bleeding tendencies, and in patients suffering organ trauma or disease – the process of fibrinolysis can result in excessive haemorrhage, making the use of anti-fibrinolytic medications potentially of clinical use. Examples of such conditions include cerebral contusion, pulmonary contusion, and liver contusion following blunt force trauma, surgery of the larynx, pharynx and other vascular soft tissues, and in the management of severe thrombocytopaenia, among others1,2.
What is Tranexamic Acid?
The anti-thrombolytic drug tranexamic acid is a synthetic derivative of the amino acid lysine. It reversibly binds to lysine binding sites on plasminogen. Although plasminogen can still be converted to plasmin in the presence of a plasminogen activator, such as tissue plasminogen activator, after binding to tranexamic acid, it can no longer interact with and digest fibrin, thereby inhibiting the dissolution of fibrin clots1.
Tranexamic acid may also directly inhibit plasmin and partially inhibit fibrinogenolysis at higher concentrations. It also reduces the inflammatory response following tissue injury or surgery, by inhibiting plasmin‐mediated activation of complement, monocytes, and neutrophils1.
Tranexamic acid is minimally metabolised in the liver, and is predominantly excreted in the urine, and has low protein binding (3%) with the majority of protein binding being to plasminogen1.
Why should we consider using Tranexamic Acid?
A comprehensive review of the randomized trials using tranexamic acid in humans undergoing elective surgery showed tranexamic acid treatment led to a reduction in transfusion requirements by a third over non-treated controls; and in trauma patients, all-cause mortality rate and bleeding-associated deaths were significantly lower in tranexamic acid-treated patients3. These data support investigation on the clinical use of tranexamic acid in dogs and cats.
When could we consider using Tranexamic Acid?
Indications for use in veterinary medicine lack published evidence for the most part. However, tranexamic acid may have theoretical benefits in the following scenarios, based on mechanism of action, and/or extrapolation from human studies1,2 —
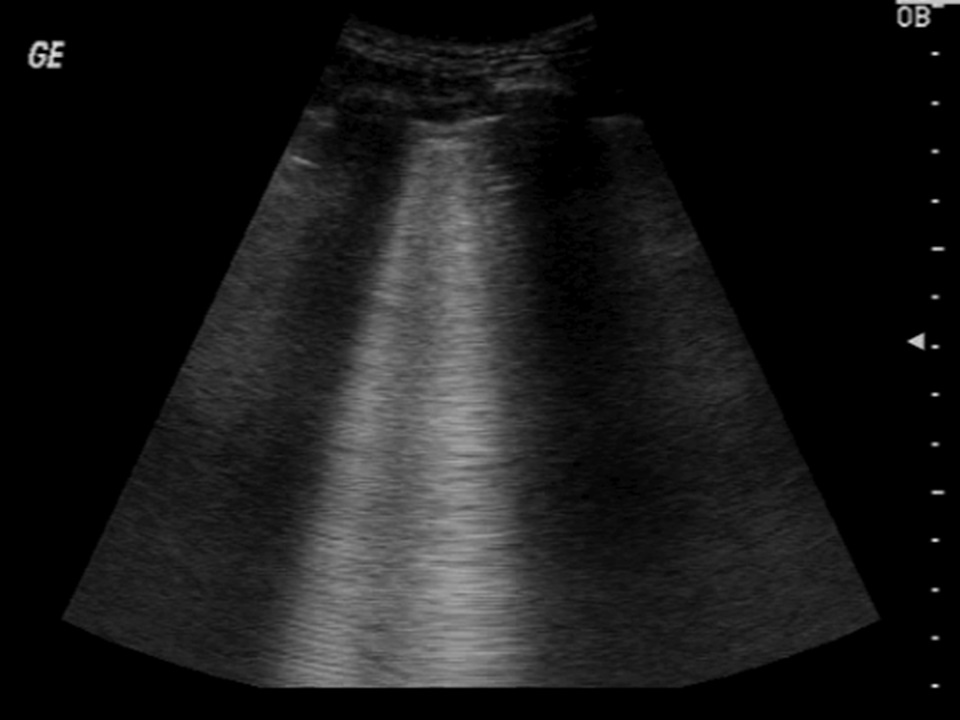
Lung ultrasound of a dog following chest trauma, showing prominent B-lines, suggestive of pulmonary contusions.
Management of post‐trauma haemorrhage
Cranio‐cerebral trauma/cerebral contusions
Pulmonary contusions
Spinal injury
Blunt force abdominal trauma
Traumatic abdominal haemorrhage
Adjunctive management of trauma‐related coagulopathy
Adjunctive management of haemostasis in patients undergoing surgery
Oral surgery
Nasal biopsy and/or surgery (topical and/or IV administration)
Orthopaedic surgery
Spinal surgery
Liver biopsy
Immune‐mediated thrombocytopaenia
Gastrointestinal bleeding from gastric erosion/ulceration
In addition to its anti-fibrinolytic effects, tranexamic acid has also been used as an effective emetic in dogs, resulting in emesis in 92% of dogs, at doses ranging from 10-50 mg/kg3,4.
Do we have veterinary evidence?
As mentioned above, there is a lack of published evidence for the use of tranexamic acid in dogs and cats. The studies that have been conducted have involved a diverse patient group, and have been retrospective in nature, making it difficult to ascertain the true value of tranexamic acid (if at all) in any single disease condition. This point is illustrated by the two studies described below:
A retrospective study of 130 dogs with clinical bleeding, compared transfusion requirements between tranexamic acid-treated dogs, and untreated controls. The cause of bleeding in both populations included neoplasia, immune-mediated thrombocytopaenia, infectious (pyometra, septic peritonitis, metritis), toxic, trauma, surgery, and other causes. Tranexamic acid-treated dogs required fewer blood transfusions than untreated bleeding control dogs, suggesting tranexamic acid may reduce transfusion requirement. However, among dogs that were transfused, there was no difference in the number of transfusions between the groups. The authors concluded that this study may not reveal the true benefit of tranexamic acid due to the varying illnesses in the patient population, and suggested more refined, prospective studies to help determine relative benefit2.
A further study of 55 dogs with surgically managed spontaneous haemoperitoneum, found no difference in transfusion requirement between control patients, and those receiving tranexamic acid at mean dose of 20 mg/kg. Patients in the study had diagnosis of malignant neoplasia, haemangiosarcoma, benign mass and trauma. As with the previously-described study, no patient in the study group was presented for emergency surgery, and none were hyper-fibrinolytic at the time of surgery. Numerous human studies show beneficial effects of tranexamic acid in hyper-fibrinolytic states, such as might be the case in acute traumatic haemorrhage patients, and the authors cite the absence of these patients from their study population as a possible reason for their observations 5.
Tranexamic acid may be of potential use in a wide range of emergency and critical illnesses.
As mentioned above, several studies have been conducted on dogs, using tranexamic acid as an emetic with up to 92% success rate 3,4.
Tranexamic acid has also been evaluated in several studies, to determine the safety2, and coagulation alterations following administration6,7. Two studies found that a bolus of 10 mg/kg, followed by 10 mg/kg/hr over 3 hours did not significantly alter coagulation parameters in healthy dogs, and that the rate of fibrinolysis in dogs appears higher than than in humans6,7. Results of these studies suggest higher doses of tranexamic acid may be required to fully inhibit fibrinolysis in dogs7,8,9.
What dose of Tranexamic Acid is recommended?
Doses for tranexamic acid in dogs have largely been extrapolated from human medicine, and have been adjusted, based on safety and efficacy studies outlined above. However, the optimal dose for anti-fibrinolysis is yet to be determined, and may need to be higher than those stated below in order to achieve clinical effect 7,8,9.
The current dose and administration protocol is as follows:
10mg/kg is given by slow intravenous infusion (over 15‐20 minutes)
Subsequent doses
10 mg/kg slow IV every 8 hours for 24 hours OR
A continuous infusion of 10 mg/kg IV over 3‐6 hours; repeated every 8 hours for up to 24 hrs.
Evidence in humans suggests that tranexamic acid administration is of maximum benefit, and therefore should be given within the first 3 hours following acute trauma, during the period of excess fibrinolysis. A delay of greater than 6 hours before commencing treatment is associated with worse outcome in trauma patients with haemorrhage as a complication 1,2.
Nausea is the predominant adverse side effect observed following administration. Premedication with maropitant or metoclopramide may reduce nausea. Ondansetron is less effective at reducing nausea following tranexamic acid administration 4,10.
Are there any side effects?
Potential side effects following administration of tranexamic acid use include 1,2,4,511:
Seizures1
Thromboembolism
Nausea/vomiting
Hypotension
Anaphylaxis
Anaphylaxis has been reported in a single patient. Successful treatment involved intravenous fluid support, corticosteroid medication, and anti-histamine therapy.
Conclusions
Tranexamic acid is a potentially useful medication in the management of excessive bleeding caused by hyperfibrinolysis. In human medicine, tranexamic acid has proven effective in reducing mortality rates, transfusion requirements, and complications in many diseases causing haemorrhage. To date, veterinary literature is sparse in this regard. Further studies to determine the optimal dosing regime, and the effect of tranexamic acid on mortality and transfusion requirements in single illness groups, e.g. cranio-cerebral trauma, pulmonary contusions, etc., are required to provide firm guidelines. In the interim, tranexamic acid appears relatively safe to use in dogs, and its cautious use may be warranted in selected patients.
References:
McCormack PL. Tranexamic acid. Drugs. 2012 Mar 1;72(5):585-617.
Kelmer E, Marer K, Bruchim Y, Klainbart S, Aroch I, Segev G. Retrospective evaluation of the safety and efficacy of tranexamic acid (Hexakapron®) for the treatment of bleeding disorders in dogs. Isr J Vet Med. 2013 Jun 1;68(2):94-100.
Kakiuchi H, Kawarai-Shimamura A, Fujii Y, et al. Efficacy and safety of tranexamic acid as an emetic in dogs. Am J Vet Res. 2014;75(12):1099-1103.
Orito K, Kawarai-Shimamura A, Ogawa A, Nakamura A. Safety and efficacy of intravenous administration for tranexamic acid-induced emesis in dogs with accidental ingestion of foreign substances. Journal of Veterinary Medical Science. 2017:17-0463.
Sigrist, Nadja E; Olgiati, Laura; Jud Schefer, Rahel (2018). Effect of tranexamic acid on intra- and postoperative haemorrhage in dogs with surgically treated hemoperitoneum. Schweizer Archiv für Tierheilkunde, 160(5):305-312.
Kelmer E, Segev G, Papashvilli V, Rahimi‐Levene N, Bruchim Y, Aroch I, Klainbart S. Effects of intravenous administration of tranexamic acid on hematological, hemostatic, and thromboelastographic analytes in healthy adult dogs. Journal of Veterinary Emergency and Critical Care. 2015 Jul;25(4):495-501.
Fletcher DJ, Blackstock KJ, Epstein K, Brainard BM. Evaluation of tranexamic acid and ε-aminocaproic acid concentrations required to inhibit fibrinolysis in plasma of dogs and humans. American Journal of Veterinary Research. 2014 Aug;75(8):731-8.
Osekavage KE, Brainard BM, Lane SL, Almoslem M, Arnold RD, Koenig A. Pharmacokinetics of tranexamic acid in healthy dogs and assessment of its antifibrinolytic properties in canine blood. Am J Vet Res. 2018;79(10):1057-1063
Kutter, Annette P N; Kantyka, Marta E; Meira, Carolina; Bettschart-Wolfensberger, Regula; Sigrist, Nadja E (2019). Effect of 50 mg/kg intravenous tranexamic acid on coagulation assessed by rotational thromboelastometry (ROTEM) in healthy Beagle dogs. Schweizer Archiv für Tierheilkunde, 161(6):369-376.
Kantyka ME. Maropitant but not ondansetron inhibits tranexamic acid-evoked emesis: a controlled blinded randomized crossover trial (Doctoral dissertation, University of Zurich).
Choi JY, Kim JH, Han HJ. Suspected anaphylactic shock associated with administration of tranexamic acid in a dog. Journal of Veterinary Medical Science. 2019:19-0225.
Learn all about the the basic principles of genetic testing, sample collection, reliable database information, test result interpretation, and recommendations for clients.
This article will explore the presentation, pertinent pathophysiology, patient selection, treatment considerations and outcomes of medical management of canine pyometra.
This short review will focus on the concept of oxygen toxicity, and its relevance in the treatment of the trauma patient - many of whom require and are given oxygen therapy as part of their treatment regime.