Attention Members: Please avoid clicking on any unsolicited emails with attachments. If you have any concerns, please contact us at info@veteducation.com.au for clarification.
Attention Members: Please avoid clicking on any unsolicited emails with attachments. If you have any concerns, please contact us at info@veteducation.com.au for clarification.
Critical Illness-Related Corticosteroid Insufficiency (CIRCI) in Dogs
Author: Dr. Philip R Judge BVSc MVS PG Cert Vet Stud MACVSc (VECC; Medicine of Dogs)
Introduction
Critical illness-related corticosteroid insufficiency (CIRCI) is well known in human medicine1-4 and has been described in dogs as well5-8.
CIRCI is defined in humans as inadequate cellular corticosteroid activity for the severity of the patient’s critical illness, manifested by insufficient glucocorticoid-glucocorticoid receptor-mediated down regulation of pro-inflammatory transcription factors4. CIRCI is known to occur in several acute conditions including sepsis, septic shock, pneumonia, acute respiratory distress syndrome (ARDS), cardiac arrest, head injury, trauma, burns, and following major tissue injury or surgery4,7. The syndrome is currently recognised by the presence of persistent hypotension in euvolaemic patients, despite appropriate vasopressor therapy. Improvement in blood pressure following therapy with hydrocortisone is considered further proof of the existence of CIRCI. Positive response to treatment is associated with improved outcome1-8.
The aim of this review is to summarise the pathology of the hypothalamic-pituitary-adrenal (HPA) axis in critical illness, and to outline current knowledge on diagnostics and treatment of CIRCI in dogs and cats.
The systemic response to injury
Systemic inflammation is an organized response to infection, or severe tissue injury that involves three (3) main components4:
The stress-response system, which is mediated by the hypothalamic-pituitary axis (HPA) and the locus ceruleus-noradrenaline/sympathetic nervous system
Acute phase reaction to tissue injury, which results in release of inflammatory mediators, including cytokines, chemokines, prostaglandins, compliment, among others
The vital organ response (cardiac, CNS etc.)
An exaggerated systemic response to tissue injury, inflammation, or infection, is the hallmark of the systemic inflammatory response syndrome and is partly driven by an imbalance of hyperactive (acute phase) inflammatory pathways, and an under-active, or dysregulated HPA4.
A review of cortisol secretion
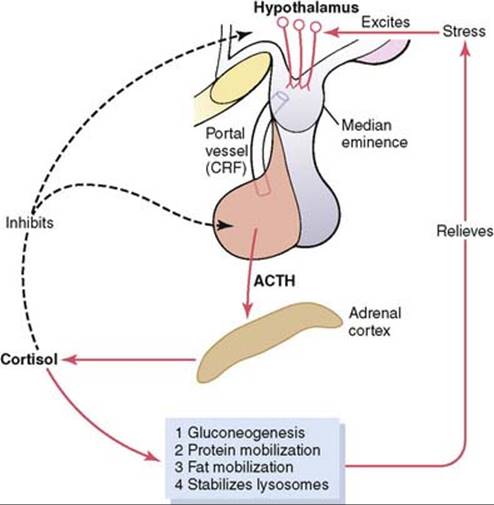
Under normal circumstances, cortisol secretion from the adrenal cortex is stimulated by release of adrenocorticotrophic hormone from the anterior pituitary gland in the brain – itself under regulatory control of corticotropin releasing hormone (CRH) in the hypothalamus – part of the HPA4.
In conditions of stress and critical illness, production of cortisol is much more complex. Acute stress induces rapid release of CRH and ACTH, under the influence of noradrenaline; and also release of arginine vasopressin from the hypothalamus, which stimulates release of ACTH as well. Additionally, in inflamed or infected tissues, inflammatory mediators directly stimulate both peripheral nerves of the autonomic nervous system (which also directly stimulate CRH), and also the adrenal cortex to produce cortisol, independent of CRH/ACTH. Furthermore, the serum half-life of cortisol increases as well, due to decreased cortisol metabolism in severe disease states. These latter two points lead to a disconnect between ACTH levels, and cortisol levels in serum in critical illness2-4. This disconnect is illustrated by two studies in humans, that showed cortisol production rates in critically ill patients were either unaltered or only marginally increased when compared to controls, despite cortisol concentrations being more markedly elevated4.
What does cortisol do?
Cortisol is a lipophilic hormone that enters the cell passively and binds to specific glucocorticoid (or mineralocorticoid) receptors within cell cytoplasm. Once bound to the receptors, the cortisol-receptor complex enters the nucleus, where it binds to specific regions on DNA to stimulate (or inhibit) gene expression – for example, inhibition or stimulation of genes associated with inflammation etc9,10. In addition, glucocorticoids can exert non-genomic effects. Specifically, in the context of the inflammatory response, they can bind to glucocorticoid receptors on vascular endothelial cell walls, inhibiting nitric oxide production9,11, and can also bind to intracellular kinase pathways to inhibit production of phospholipase enzymes within the cytoplasm. Additionally, cortisol may impair T-cell receptor signaling9.
HPA dysfunction in SIRS and Sepsis?
Despite the direct and indirect simulation of the HPA in severe illness and sepsis, adrenal cortisol synthesis either remains unchanged, or only marginally increased4. This is thought due to the following:
Damage to neuroendocrine cells within the adrenal glands resulting from adrenal haemorrhage caused by disseminated intravascular coagulation (DIC), elevated adrenal blood pressure, or ischaemia4,9.
Altered CRH/ACTH secretion: Initial stimulation of CRH and ACTH by inflammatory cytokines, including interleukin-1 is frequently associated with a progressive decline in secretion within 72 hours of the onset of sepsis, caused by over-expression of nitric oxide synthase in the hypothalamus, partly triggered by interleukin-1, and tumour necrosis factor. Subsequent production of nitric oxide leads to apoptosis of neurons in the hypothalamus and pituitary12-15.
Direct inhibition of CRH and ACTH secretion, by increasing cortisol concentrations in circulation (negative-feedback loop)3.
Reduced cortisol secretion: The adrenal gland has very limited stores of cortisol – meaning any increase in serum cortisol needs to be met by increasing adrenal gland production. The adrenal glands of patients with sepsis are known to have reduced cholesterol, which is a precursor to cortisol synthesis, and this may blunt the response of the adrenal gland to simulation16.
Medications: such as etomidate, opioids, and benzodiazepines may either diminish the cortisol response, production of cortisol by the adrenal gland, or the HPA at various points17-19.
The tissue activity of cortisol is reduced, and the half-life of cortisol appears to be increased in critical illness – suggesting reduced cortisol metabolism and breakdown3.
Tissue resistance to cortisol: Despite seemingly adequate peripheral tissue cortisol, cortisol receptor activity in the intracellular environment appears reduced in critical illness, suggesting corticosteroid resistance. Cortisol resistance is well-recognised as a complication of critical illness, including patients with sepsis, septic shock, acute respiratory distress syndrome, and other severe illnesses20.
How do I diagnose CIRCI in the dog?
The incidence of CIRCI in high-risk patients (those with hypotension, shock, or sepsis) ranges from 30-45%; and the presence of CIRCI in both humans and dogs appears to result in increased risk of morbidity and mortality in critical illness – making a diagnosis of critical importance in patient management21.
Baseline cortisol concentrations, ACTH concentrations, and ACTH stimulation tests have all been used to differentiate patients likely to have CIRCI (and who may benefit from provision of exogenous corticosteroids) and those who do not. Whilst some studies show a higher serum cortisol concentration in non-surviving critically ill dogs22, other studies show poor predictive value of cortisol as a single measure of predicting CIRCI23. Responsiveness to ACTH administration appears to offer the greatest degree of accuracy in terms of predicting patients who require both vasopressor therapy, and those who may benefit from exogenous corticosteroid therapy2-7, 23.
A study carried out on 48 acute critically ill dogs revealed that dogs with a change in cortisol concentration following ACTH administration of less than 83 nmol/L were more likely to need vasopressor therapy as part of their treatment plan5. It was postulated that these patients may have CIRCI and therefore may benefit from glucocorticoid replacement.
A further study of 33 septic dogs admitted to a small animal intensive care unit had serum cortisol concentrations, ACTH concentrations and ACTH stimulation tests performed. Dogs with a change in cortisol concentration of less than 80 nmol/L were more likely to have hypotension, and were less likely to survive to discharge, being 4.1 times more likely to die7. Again, it is possible these patients may have CIRCI, and therefore may benefit from glucocorticoid replacement.
However, a study of 21 dogs with systemic inflammatory response syndrome (SIRS) and critical illness that looked at cortisol change and mortality, found that only hypotension and elevated basal cortisol concentrations were predictive of mortality, and that delta cortisol, following ACTH stimulation, was not predictive of survival24.
Because of uncertainty regarding how to appropriately diagnose CIRCI in humans, the human critical care community does not advocate any method of diagnosis for CIRCI at present. Essentially, the “diagnosis” of CIRCI in people is currently made by evaluating response to treatment with low-dose hydrocortisone, in patients in whom vasopressors have failed to improve blood pressure, without assessment of the hypothalamic-pituitary-adrenal (HPA) axis. This is currently the approach in canine (and feline) critical care medicine also25.
Treatment of CIRCI
Because of the increase in morbidity and mortality associated with suspected CIRCI in people, therapy is pursued in most patient with persistent hypotension, despite being volume replete, and who have poor response to vasopressor therapy25.
Most references suggest that CIRCI in people can be treated using physiological doses of corticosteroids, equivalent to prednisolone dose of 1 mg/kg25. As stated above, treatment is recommended in patients who are volume replete (non-hypovolaemic, non-dehydrated) patients who remain hypotensive, despite appropriate therapy with vasopressors, such as noradrenaline and dopamine3,25.
In animals, the treatment recommendations are less clear – owing primarily to lack of published evidence on effective dosing. The criteria for the diagnosis of CIRCI are currently extrapolated from human medicine, and as such, patients with severe illness, who are hypotensive despite normal blood volume and the use of vasopressor therapy, are considered for therapy. Currently published case reports and case series of dose rates and duration of therapy for CIRCI in dogs are outlined below:
A single case report in a dog with pressor-refractory septic shock describes the use of hydrocortisone at 0.5 mg/kg IV q 6 hrs. to treat suspected CIRCI. Pressors were discontinued within hours of starting the hydrocortisone, and the steroid dose was tapered over many days beginning 4 days after pressor independence26.
One small study in 8 dogs with septic shock administered the treatment group hydrocortisone 1 mg/kg IV q 6 hrs. for 5 days, with a 6-day tapering regimen25.
A single case report in a critically ill cat describes the use of dexamethasone 0.08 mg/kg IV q24h to treat fluid-loaded, pressor-dependent hypotension. It should be noted that dexamethasone is currently not recommended, owing to greater potential for gastrointestinal adverse effects, and immunosuppression, when compared to hydrocortisone27.
A 27-month-old female cat was presented with septic peritonitis secondary to a ruptured pyometra and subsequent pyothorax. Vasopressor-refractory septic shock led to a suspicion of critical illness-related corticosteroid insufficiency, successfully treated with intravenous hydrocortisone 1 mg/kg IV bolus, followed by continuous infusion of 0.16 mg/kg/hr28.
Summaries of these studies have extrapolated therapeutic doses of hydrocortisone for dogs and cats as follow:
Hydrocortisone 1-4 mg/kg/day – divided into 4 equal IV doses, given every 6 hrs, or delivered as a continuous infusion OR
Hydrocortisone 0.5 mg/kg IV q 4 hrs OR
Hydrocortisone 0.08-1.2 mg/kg/hr continuous infusion for 24 hrs
No clear protocols exist for the suggested length of treatment, or for weaning patients from hydrocortisone following the initial 24 hr period. Extrapolation from human critical care suggests treatment may be required for up to 3-4 days (or longer, depending on disease) at the above-recommended doses, followed by gradual reduction in dose over subsequent 3-4 days25, or dose reduction of 50% every 48 hrs of treatment28.
Prognosis
The prognosis HPA axis function recovery for patients that recover from their critical illness following an episode of CIRCI is very good25.
Looking to the future
Given the loose diagnostic criteria currently applied to the diagnosis of CIRCI, it is clear that further research into the aetiopathogenesis and diagnostic accuracy of the condition will benefit the patient population at risk. Furthermore, research on appropriate therapy is also warranted, to improve potential benefit, whilst reducing risk to affected patients.
References
Beishuizen A, Thijs LG, Vermes I. Decreased levels of dehydroepiandrosterone sulphate in severe critical illness: a sign of exhausted adrenal reserve? Critical Care. 2002 Oct 1;6(5):434.
Venkatesh, B. Cohen, J. (2011): Adrenocortical (dys)function is septic shock – A sick euadrenal state. Best Pract. Res. Clin. Endocrinol. Metab. 25, 719–733.
Marik PE. Critical illness-related corticosteroid insufficiency. Chest. 2009 Jan 1;135(1):181-93.
Annane D, Pastores SM, Arlt W, Balk RA, Beishuizen A, Briegel J, Carcillo J, Christ-Crain M, Cooper MS, Marik PE, Meduri GU. Critical illness-related corticosteroid insufficiency (CIRCI): a narrative review from a Multispecialty Task Force of the Society of Critical Care Medicine (SCCM) and the European Society of Intensive Care Medicine (ESICM). Intensive care medicine. 2017 Dec 1;43(12):1781-92.
Martin, L. G., Groman, R. P., Fletcher, D. J., Behrend, E. N., Kemppainen, R. J., Moser, V. R. and Hickey, K. C. (2008): Pituitary-adrenal function in dogs with acute critical illness. JAVMA 233, 87–95.
Goy-Thollot, I., Decosne-Junot, C. and Bonnet, J-M. (2006): Adrenal responsiveness in critically ill dogs: prospective study. Rev. Méd. Vét. 157, 213–218.
Burkitt, J. M., Haskins, S. C., Nelson, R. W. and Kass, P. H. (2007): Relative adrenal insufficiency in dogs with sepsis. JVIM 21, 226–231.
Burkitt Creedon, J. M. (2015): Controversies surrounding critical illness-related corticosteroid insufficiency in animals. J. Vet. Emerg. Crit. Care 25, 107–112.
Goodwin JE, Feng Y, Velazquez H, et al: Endothelial glucocorticoid receptor is required for protection against sepsis. Proc Natl Acad Sci U S A 2013; 110:306–311
Mélik Parsadaniantz S, Levin N, Lenoir V, et al: Human interleukin 1 beta: corticotropin releasing factor and ACTH release and geneexpression in the male rat: in vivo and in vitro studies. J Neurosci Res 1994; 37:675–682
Parsadaniantz SM, Batsché E, Gegout-Pottie P, et al: Effects of continuous infusion of interleukin 1 beta on corticotropin-releasing hormone (CRH), CRH receptors, proopiomelanocortin gene expression and secretion of corticotropin, beta-endorphin and corticosterone. Neuroendocrinology 1997; 65:53–63
Wong ML, Rettori V, al-Shekhlee A, et al: Inducible nitric oxide synthase gene expression in the brain during systemic inflammation. Nat Med 1996; 2:581–584
Sharshar T, Gray F, Lorin de la Grandmaison G, et al: Apoptosis of neurons in cardiovascular autonomic centres triggered by inducible nitric oxide synthase after death from septic shock. Lancet 2003; 362:1799–1805
Annane D, Maxime V, Ibrahim F, et al: Diagnosis of adrenal insufficiency in severe sepsis and septic shock. Am J Respir Crit Care Med 2006; 174:1319–1326
Bruder EA, Ball IM, Ridi S, et al: Single induction dose of etomidate versus other induction agents for endotracheal intubation in critically ill patients. Cochrane Database Syst Rev 2015; 1:CD010225
Daniell HW: Opioid contribution to decreased cortisol levels in critical care patients. Arch Surg 2008; 143:1147–1148
Thomson I, Fraser R, Kenyon CJ: Regulation of adrenocortical steroidogenesis by benzodiazepines. J Steroid Biochem Mol Biol 1995; 53:75–79
Dendoncker K, Libert C: Glucocorticoid resistance as a major drive in sepsis pathology. Cytokine Growth Factor Rev 2017; 35:85–96
Marik PE, Zaloga GP. Adrenal insufficiency during septic shock. Crit Care Med 2003;31:141–145.
Swales H, Batchelor DJ, O’Connell EM. Evaluation of serum cortisol concentration as a prognostic indicator for nonsurvival to hospital discharge in critically ill dogs. Journal of the American Veterinary Medical Association. 2020 May 1;256(9):1034-40.
Sweeney DA, Natanson C, Banks SM, Solomon SB, Behrend EN. Defining normal adrenal function testing in the intensive care unit setting: a canine study. Critical care medicine. 2010 Feb;38(2):553.
Pierini A, Marchetti M, Favilla G, Gori E, Lippi I, Ceccherini G, Marchetti V. Critical illness-related corticosteroid insufficiency (CIRCI) in dogs with systemic inflammatory response syndrome (SIRS).
Creedon JM. Controversies surrounding critical illness‐related corticosteroid insufficiency in animals. Journal of Veterinary Emergency and Critical Care. 2015 Jan;25(1):107-12.
Peyton JL, Burkitt JM. Critical illness-related corticosteroid insufficiency in a dog with septic shock. J Vet Emerg Crit Care 2009; 19:262–268.
Durkan S, de Laforcade A, Rozanski E, et al. Suspected relative adrenal insufficiency in a critically ill cat. J Vet Emerg Crit Care 2007; 17:197–201.
Pisano SR, Howard J, Posthaus H, Kovacevic A, Yozova ID. Hydrocortisone therapy in a cat with vasopressor‐refractory septic shock and suspected critical illness‐related corticosteroid insufficiency. Clinical case reports. 2017 Jul;5(7):1123.
RACE-approved for 20 CPD Points
Endocrine Emergencies in Small Animal Practice
4-Week Interactive and Tutor-Guided Course for Veterinarians
Endocrine emergencies encompass a wide range of diseases – including diabetic ketoacidosis, hypothyroid coma, hypoadrenocorticism and catastrophic abdominal haemorrhage from pheochromocytoma, to name a few.
This 4-week course will delve into the most common endocrine emergencies seen in small animal practice – reviewing the most recent literature, to present a concise account of these important diseases, and how you, as a clinician, can achieve the best outcome for your patient.
Learn all about the the basic principles of genetic testing, sample collection, reliable database information, test result interpretation, and recommendations for clients.
This article will explore the presentation, pertinent pathophysiology, patient selection, treatment considerations and outcomes of medical management of canine pyometra.
This short review will focus on the concept of oxygen toxicity, and its relevance in the treatment of the trauma patient - many of whom require and are given oxygen therapy as part of their treatment regime.